
Shopping Cart
- Remove All
 Your shopping cart is currently empty
Your shopping cart is currently empty


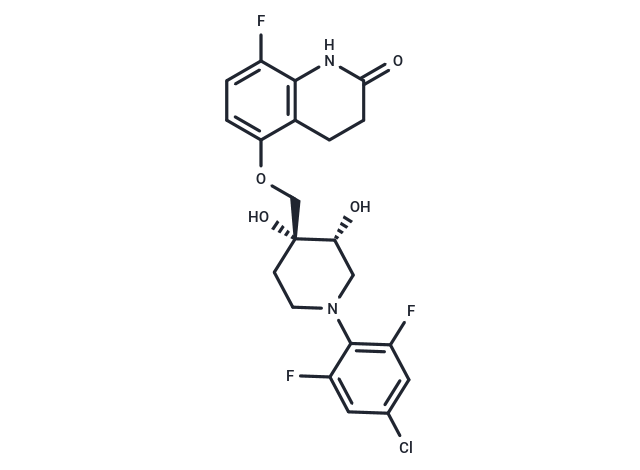
OPC-167832 is a potent and orally active dprE1 Inhibitor with an IC50 of 0.258 μM. OPC-167832 has antituberculosis activity and can be used for the research of tuberculosis caused by Mycobacterium tuberculosis[1].
| Pack Size | Price | Availability | Quantity |
|---|---|---|---|
| 25 mg | $1,170 | 10-14 weeks | |
| 50 mg | $1,530 | 10-14 weeks | |
| 100 mg | $2,440 | 10-14 weeks |
| Description | OPC-167832 is a potent and orally active dprE1 Inhibitor with an IC50 of 0.258 μM. OPC-167832 has antituberculosis activity and can be used for the research of tuberculosis caused by Mycobacterium tuberculosis[1]. OPC-167832 exhibits very low MICs against laboratory strains of M. tuberculosis H37Rv (MIC: 0.0005 μg/ml) and Kurono (MIC: 0.0005 μg/ml) and strains with monoresistance to rifampin (RIF), isoniazid (INH), ethambutol (EMB), streptomycin (STR), and pyrazinamide (PZA) (MIC: 0.00024-0.001 μg/ml). However, OPC-167832 has minimal or no activity against standard strains of nonmycobacterial aerobic and anaerobic bacteria[1].The IC90 values of OPC-167832 against intracellular M. tuberculosis strains H37Rv and Kurono are 0.0048 and 0.0027 μg/ml, respectively. OPC-167832 shows bactericidal activity against intracellular M. tuberculosis at a low concentration, and the bactericidal activity is saturated at concentrations of 0.004 μg/ml or higher[1]. OPC-167832 (oral administration; 0.625-10 mg/kg) exhibits a good pharmacokinetic characteristic. The plasma reaches peak at 0.5 h to 1.0 h (tmax) and is eliminated with a half-life (t1/2) of 1.3 h to 2.1 h OPC-167832 distribution in the lungs is approximately 2 times higher than that in plasma, and the Cmax and AUCt of OPC-167832 in plasma and the lungs shows dose dependency[1].OPC-167832 (oral administration; 0.625-10 mg/kg; 4 weeks) significantly reduces lung CFU compared to the vehicle group. The dose-dependent decrease of lung CFU is observed from 0.625 mg/kg to 2.5 mg/kg. In a M. tuberculosis Kurono-infected ICR female mice model. OPC-167832 combines with DMD, BDQ, or LVX via oral gavage exhibits significantly higher efficacies than each single agent alone[1].[1].OPC-167832 (oral gavage; 2.5 mg/kg; combination with DCMB; 12 weeks) demonstrates the most potent efficacy when compares with DC, DCB. The lung CFU count after 6 weeks of treatment is below the detection limit, and at the end of just 8 weeks of treatment, the bacteria in the lungs of all the evaluated mice had already been eradicate[1]. [1]. Norimitsu Hariguchi, et al. OPC-167832, a Novel Carbostyril Derivative with Potent Antituberculosis Activity as a DprE1 Inhibitor.Antimicrob Agents Chemother. 2020 May 21;64(6):e02020-19. |
| In vitro | OPC-167832 exhibits very low MICs against laboratory strains of M. tuberculosis H37Rv (MIC: 0.0005 μg/ml) and Kurono (MIC: 0.0005 μg/ml) and strains with monoresistance to rifampin (RIF), isoniazid (INH), ethambutol (EMB), streptomycin (STR), and pyrazinamide (PZA) (MIC: 0.00024-0.001 μg/ml). However, OPC-167832 has minimal or no activity against standard strains of nonmycobacterial aerobic and anaerobic bacteria[1].The IC90 values of OPC-167832 against intracellular M. tuberculosis strains H37Rv and Kurono are 0.0048 and 0.0027 μg/ml, respectively. OPC-167832 shows bactericidal activity against intracellular M. tuberculosis at a low concentration, and the bactericidal activity is saturated at concentrations of 0.004 μg/ml or higher[1]. |
| In vivo | OPC-167832 (oral administration; 0.625-10 mg/kg) exhibits a good pharmacokinetic characteristic. The plasma reaches peak at 0.5 h to 1.0 h (tmax) and is eliminated with a half-life (t1/2) of 1.3 h to 2.1 h OPC-167832 distribution in the lungs is approximately 2 times higher than that in plasma, and the Cmax and AUCt of OPC-167832 in plasma and the lungs shows dose dependency[1].OPC-167832 (oral administration; 0.625-10 mg/kg; 4 weeks) significantly reduces lung CFU compared to the vehicle group. The dose-dependent decrease of lung CFU is observed from 0.625 mg/kg to 2.5 mg/kg. In a M. tuberculosis Kurono-infected ICR female mice model. OPC-167832 combines with DMD, BDQ, or LVX via oral gavage exhibits significantly higher efficacies than each single agent alone[1].[1].OPC-167832 (oral gavage; 2.5 mg/kg; combination with DCMB; 12 weeks) demonstrates the most potent efficacy when compares with DC, DCB. The lung CFU count after 6 weeks of treatment is below the detection limit, and at the end of just 8 weeks of treatment, the bacteria in the lungs of all the evaluated mice had already been eradicate[1]. |
| Molecular Weight | 456.84 |
| Formula | C21H20ClF3N2O4 |
| Cas No. | 1883747-71-4 |
| Storage | Powder: -20°C for 3 years | In solvent: -80°C for 1 year | Shipping with blue ice. | |||||||||||||||||||||||||||||||||||
| Solubility Information | DMSO: 180 mg/mL (394.01 mM), Sonication is recommended. | |||||||||||||||||||||||||||||||||||
Solution Preparation Table | ||||||||||||||||||||||||||||||||||||
DMSO
| ||||||||||||||||||||||||||||||||||||
 For example, your dosage is 10 mg/kg Each animal weighs 20 g, and the dosage volume is 100 μL . A total of 10 animals were administered, and the formula you used is 5%
For example, your dosage is 10 mg/kg Each animal weighs 20 g, and the dosage volume is 100 μL . A total of 10 animals were administered, and the formula you used is 5%  DMSO+30% PEG300+5% Tween 80+60% ddH2O. So your working solution concentration is 2 mg/mL。 (mother liquor concentration of 40 mg/mL), if you need to configure a concentration that exceeds the solubility of the product, please contact us first. main solution, add 300 μLPEG300 mix well and clarify, then add 50 more μL Tween 80, mix well and clarify, then add 600 more μLddH2O mix well and clarify
DMSO+30% PEG300+5% Tween 80+60% ddH2O. So your working solution concentration is 2 mg/mL。 (mother liquor concentration of 40 mg/mL), if you need to configure a concentration that exceeds the solubility of the product, please contact us first. main solution, add 300 μLPEG300 mix well and clarify, then add 50 more μL Tween 80, mix well and clarify, then add 600 more μLddH2O mix well and clarify Hello! How can I help you today?
Hello! How can I help you today? 
Copyright © 2015-2025 TargetMol Chemicals Inc. All Rights Reserved.